A CASE OF PRIMARY IMMUNODEFICIENCY DISORDER
- The following E-log aims at discussing our patient de-identified health data shared after taking the guardian's signed consent.
- Here we discuss our individual patient problems through series of inputs from available global online community of experts with an aim to solve the patients clinical problem with current best evidence based input.
- This E-log also reflects my patient's centered online learning portfolio.
I have been given this case to solve in an attempt to understand the topic of "Patient Clinical Data Analysis" to develop my competency in reading and comprehending clinical data including history, clinical findings, investigations and come up with a diagnosis and providing treatment best to our skills and wisdom.
HISTORY OF PAST ILLNESS
➤Not a known case of hypertension , diabetes ,bronchial asthma ,epilepsy, tuberculosis
➤k/c/o common variable immunodeficiency with Autoimmune hemolytic anemia.
DRUG HISTORY
➤Immunoglobulin injection since 2020
➤Blood transfusion 1year back (3 units)
PERSONAL HISTORY
➤Student
➤Patient is unmarried
➤Patient takes mixed diet but has a normal appetite.
➤Bowel and bladder movement is normal and regular.
➤Menarche at 15yrs
FAMILY HISTORY
➤No significant family history.
GENERAL EXAMINATION
➤Pallor : Not seen
➤Icterus : Not seen
➤Cyanosis : Not seen
➤Clubbing : Not seen
➤Lymphadenopathy : Not seen
➤Edema : Not seen
➤Weight : 28
➤Height: 4'5''
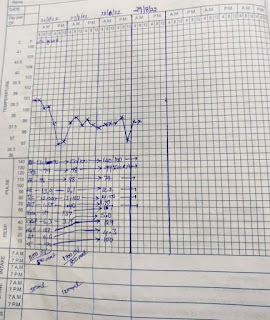
VITALS
➤Temperature : 98.3℉
➤PR : 120 beats per minute
➤BP : systolic 80mm hg by palpatory method
➤RR : 24 cycles per minute
➤SpO2 : 97% in room air
➤Blood Sugar (random) : 112mg/dl
SYSTEMIC EXAMINATION
CARDIOVASCULAR SYSTEM EXAMINATION
➤s1 and s2 heard
➤Thrills absent.,
➤No cardiac murmurs
RESPIRATORY SYSTEM
➤Normal vesicular breath sounds heard.
➤Bilateral air entry present
➤Trachea is in midline
ABDOMINAL EXAMINATION
INSPECTION
➤Shape - Scaphoid
➤Equal movements in all the quadrants.
➤No visible pulsation, dilated veins and localized swellings.
PALPATION
➤Tenderness in right iliac fossa
➤No palpable mass
CENTRAL NERVOUS SYSTEM EXAMINATION
➤Conscious and coherent
PROVISIONAL DIAGNOSIS : ACUTE GASTROENTRITIS K/C/O PRIMARY IMMUNODEFICIENCY DISORDER
INVESTIGATIONS :
DAY 1
 |
| LYMPHOCYTES 11% |
 |
| NORMAL |
 |
| ELEVATED 42mm/hour |
 |
| BLOOD IS SEEN |
 |
| POSITIVE 1.2mg/dl |
 |
| CREATININE 1.1mg/dl CALCIUM 7.3mg/dl |
 |
| TOTAL BILIRUBIN:4.41mg/dl DIRECT BILIRUBIN:0.89mg/dl |
 |
| BOWEL WALL EDEMA SPLENOMEGALY |
 |
 |
| PLENTY OF PUS CELLS NO OVA/CYSTS SEEN |

TREATMENT
1) IV FLUIDS NS AND RL 75ML/HR
2) TAB. ZOFER 4MG PO/OD
3) TAB PANTOP 40MG PO/OD
4) TAB PARACETAMOL 650MG PO/SOS
5) TAB SPOROLAC DS PO/TID
DAY 2
➤Loose stools decreased
➤No fever spikes
TREATMENT
1)IV FLUIDS NS AND RL 75ML/HR
2) TAB PANTOP 40MG PO/OD
3) TAB PARACETAMOL 500MG PO/SOS
4) TAB SPOROLAC 2tab PO/TID
5) PLENTY OF ORAL FLUIDS
6) ORS ONE SACHET IN 1LTR WATER PO/TID
7) BP/PR/TEMP 4th HOURLY
DAY 3
➤Loose stools decreased
➤No fever spikes
TREATMENT
1) IV FLUIDS NS AND RL 50ML/HR
2) TAB PANTOP 40MG PO/OD
3) TAB PARACETAMOL 500MG PO/SOS
4) TAB SPOROLAC 2tab PO/TID
5) PLENTY OF ORAL FLUIDS
6) ORS ONE SACHET IN 1LTR WATER PO/TID
7) BP/PR/TEMP 4th HOURLY
DAY 4
➤Loose stools decreased
➤No fever spikes
TREATMENT
1) IV FLUIDS NS AND RL 50ML/HR
2) TAB PANTOP 40MG PO/OD
3) TAB PARACETAMOL 500MG PO/SOS
4) TAB SPOROLAC 2tab PO/TID
5) PLENTY OF ORAL FLUIDS
6) ORS ONE SACHET IN 1LTR WATER PO/TID
7) BP/PR/TEMP 4th HOURLY
DAY 5
➤Loose stools decreased
➤No fever spikes
TREATMENT
1) IV FLUIDS NS AND RL 50ML/HR
2) TAB PANTOP 40MG PO/OD
3) TAB PARACETAMOL 500MG PO/SOS
4) TAB SPOROLAC 1tab PO/TID
5) PLENTY OF ORAL FLUIDS
6) ORS ONE SACHET IN 1LTR WATER PO/TID
7) BP/PR/TEMP 4th HOURLY
8) TAB OFLOX-OZ PO/BD
9) SYP. POTKLOR 10ML ONE GLASS OF WATER PO/BD


Comments
Post a Comment